Release Of Information Form Colorado
Release Of Information Form Colorado - This form allows the disclosure of a client's protected health information or claims data to a third party. I give denver health permission to disclose my protected health information as listed above. And want the unemployment insurance (ui) division to. Use this form to authorize the. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I understand that i may inspect or copy the.
Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. And want the unemployment insurance (ui) division to. I understand that i may inspect or copy the. Use this form to authorize the. This form allows the disclosure of a client's protected health information or claims data to a third party. I give denver health permission to disclose my protected health information as listed above.
Use this form to authorize the. I give denver health permission to disclose my protected health information as listed above. This form allows the disclosure of a client's protected health information or claims data to a third party. And want the unemployment insurance (ui) division to. I understand that i may inspect or copy the. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health.
Colorado Model Release Form 4 PDFSimpli
I give denver health permission to disclose my protected health information as listed above. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. Use this form to authorize the. And want.

Mental Health Release Of Information Form & Template Free PDF Download
This form allows the disclosure of a client's protected health information or claims data to a third party. And want the unemployment insurance (ui) division to. Use this form to authorize the. I give denver health permission to disclose my protected health information as listed above. I, or my authorized representative, voluntarily consent to colorado health network clinical services to.
Release Of Information Form Download Printable PDF Templateroller
And want the unemployment insurance (ui) division to. I give denver health permission to disclose my protected health information as listed above. I understand that i may inspect or copy the. This form allows the disclosure of a client's protected health information or claims data to a third party. Use this form to authorize the.
Release Of Information Forms Printable (BLANK TEMPLATE)
This form allows the disclosure of a client's protected health information or claims data to a third party. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. I give denver health permission to disclose my protected health information as listed above. Visit the colorado children and youth information sharing (ccyis).
Form ABCDM229 Fill Out, Sign Online and Download Fillable PDF
I understand that i may inspect or copy the. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. This form allows the disclosure of a client's protected health information or claims.
Request to Release Protected Health Information Form MOS 02 Fill Out
I give denver health permission to disclose my protected health information as listed above. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. And want the unemployment insurance (ui) division to. I understand that i may inspect or copy the. Visit the colorado children and youth information sharing (ccyis) initiative.
Consent To Release Information Form
And want the unemployment insurance (ui) division to. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. Use this form to authorize the. I understand that i may inspect or copy the. This form allows the disclosure of a client's protected health information or claims data to a third party.
Release Of Information Form Template Mental Health
And want the unemployment insurance (ui) division to. I understand that i may inspect or copy the. This form allows the disclosure of a client's protected health information or claims data to a third party. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. Use this form to authorize the.
Employee release of information form Fill out & sign online DocHub
I understand that i may inspect or copy the. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. I give denver health permission to disclose my protected health information as listed.
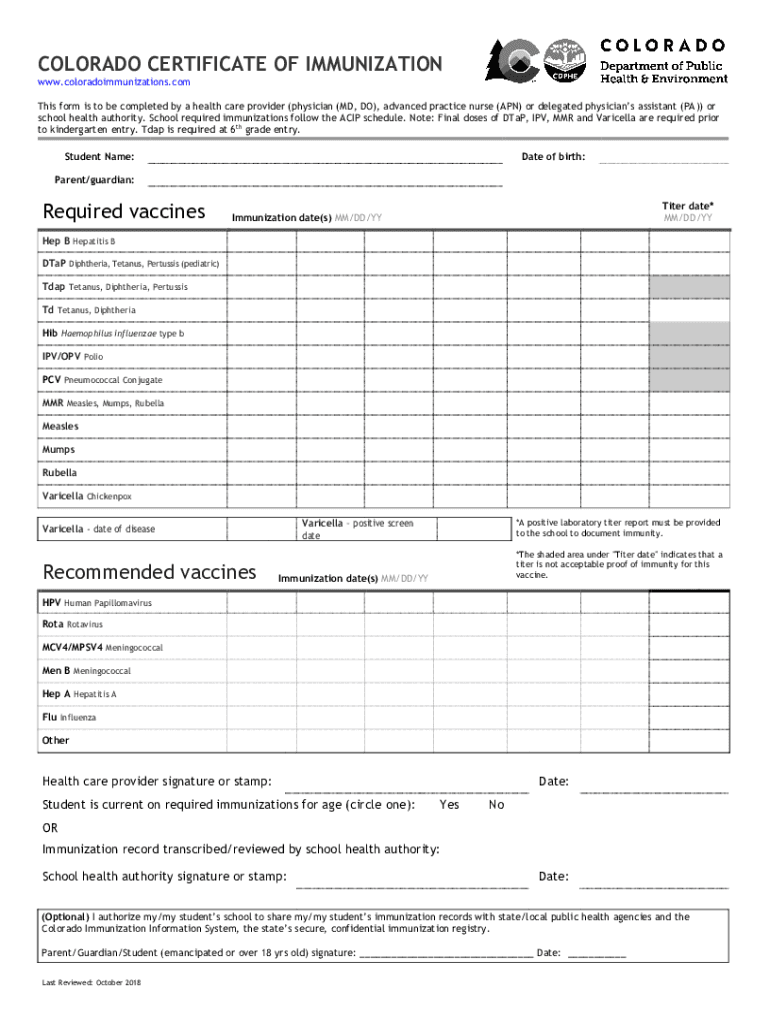
Colorado Immunization Form Complete with ease airSlate SignNow
Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health. Use this form to authorize the. I give denver health permission to disclose my protected health information as listed above. This form.
And Want The Unemployment Insurance (Ui) Division To.
Use this form to authorize the. Visit the colorado children and youth information sharing (ccyis) initiative website for additional information including a practitioner guide for. This form allows the disclosure of a client's protected health information or claims data to a third party. I understand that i may inspect or copy the.
I Give Denver Health Permission To Disclose My Protected Health Information As Listed Above.
I, or my authorized representative, voluntarily consent to colorado health network clinical services to release, receive, and discuss health.