Release Information Consent Form
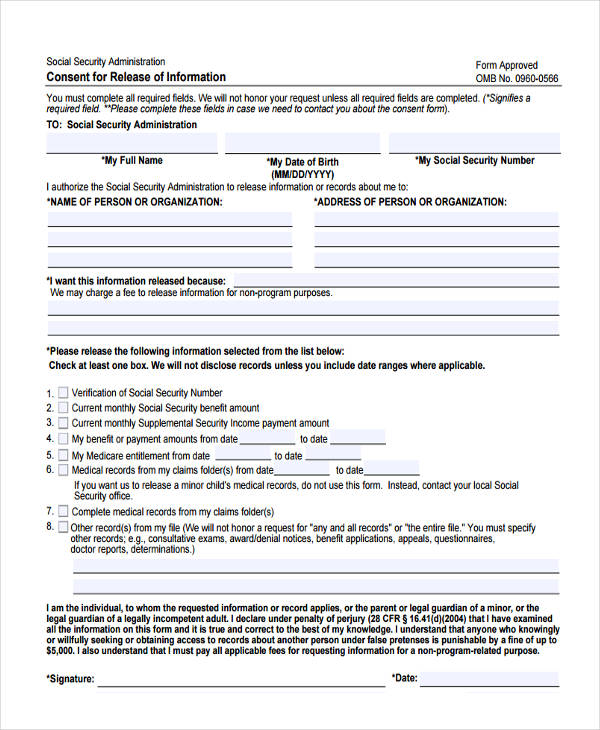
Release Information Consent Form - This form will allow us to share certain health information about you with a family member or other trusted person. This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Sample authorization for release of confidential information. Only complete this form if you.
Sample authorization for release of confidential information. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; This consent form will expire on (date)_____________ or __________ days from the. Only complete this form if you. This form will allow us to share certain health information about you with a family member or other trusted person.
The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; This form will allow us to share certain health information about you with a family member or other trusted person. This consent form will expire on (date)_____________ or __________ days from the. Only complete this form if you. Sample authorization for release of confidential information.
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
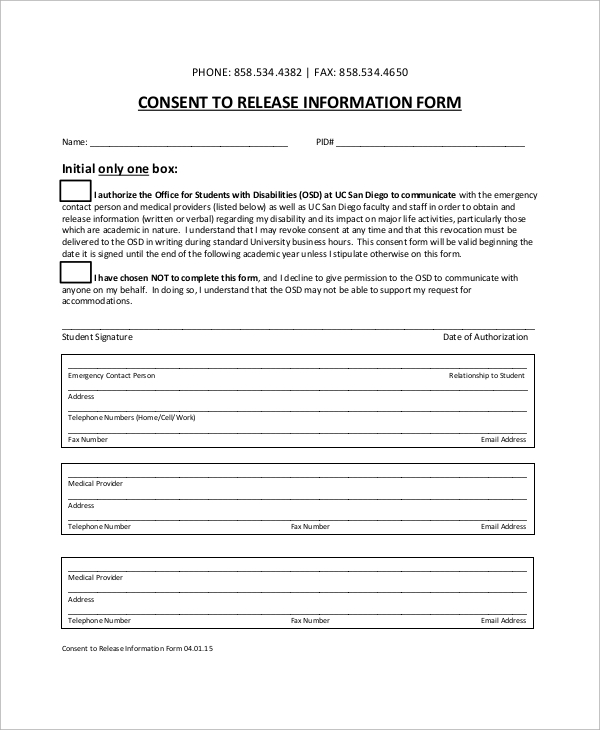
This form will allow us to share certain health information about you with a family member or other trusted person. This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Only complete this form if you..

Free Consent Forms (22) Sample Word PDF eForms
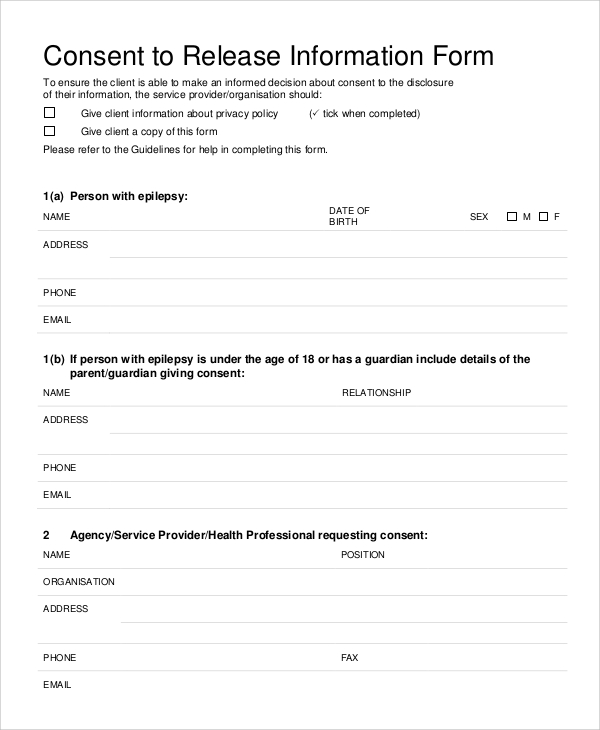
This form will allow us to share certain health information about you with a family member or other trusted person. Sample authorization for release of confidential information. This consent form will expire on (date)_____________ or __________ days from the. Only complete this form if you. The form authorizes release of information in accordance with the health insurance portability and accountability.
FREE 9+ Sample Release of Information Forms in MS Word PDF
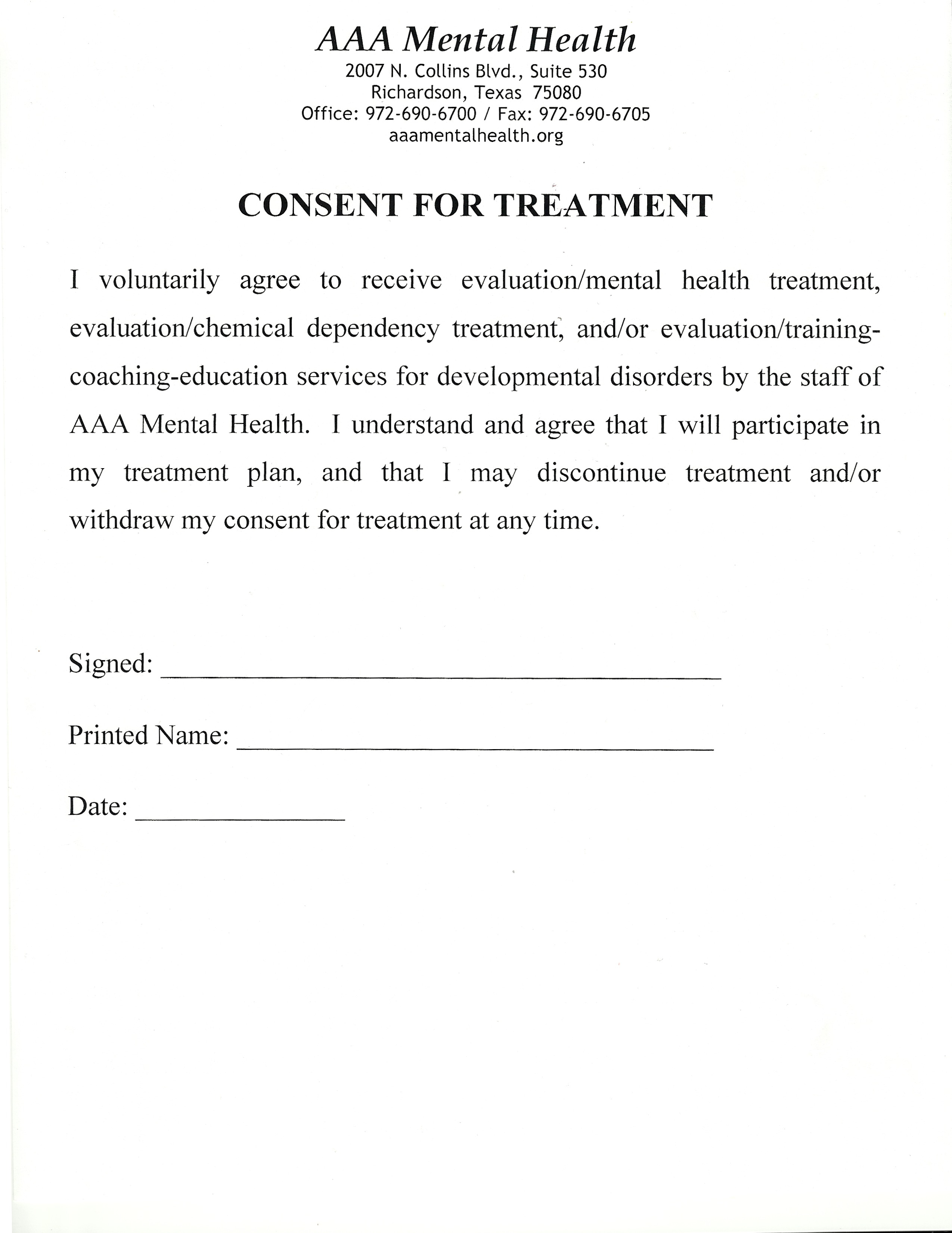
The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Only complete this form if you. This consent form will expire on (date)_____________ or __________ days from the. This form will allow us to share certain health information about you with a family member or other trusted person..

Free Consent Forms (22) Sample Word PDF eForms
Only complete this form if you. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Sample authorization for release of confidential information. This consent form will expire on (date)_____________ or __________ days from the. This form will allow us to share certain health information about you with.
FREE 9+ Sample Informed Consent Forms in PDF MS Word
This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; This form will allow us to share certain health information about you with a family member or other trusted person. Sample authorization for release of confidential.
Medical Consent Letter Template Samples Letter Template Collection
Sample authorization for release of confidential information. Only complete this form if you. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; This form will allow us to share certain health information about you with a family member or other trusted person. This consent form will expire.
Authorization to Release Loan Information Fill and Sign Printable
This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Only complete this form if you. This form will allow us to share certain health information about you with a family member or other trusted person..
FREE 9+ Release Of Medical Information Form Samples in MS Word PDF
Sample authorization for release of confidential information. This form will allow us to share certain health information about you with a family member or other trusted person. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Only complete this form if you. This consent form will expire.
FREE 12+ Sample Medical Release Forms in PDF MS Word Excel
This form will allow us to share certain health information about you with a family member or other trusted person. Sample authorization for release of confidential information. Only complete this form if you. This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability.

Consent Bookkeeping Fill Online, Printable, Fillable, Blank pdfFiller
Only complete this form if you. This form will allow us to share certain health information about you with a family member or other trusted person. This consent form will expire on (date)_____________ or __________ days from the. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164;.
The Form Authorizes Release Of Information In Accordance With The Health Insurance Portability And Accountability Act, 45 Cfr Parts 160 And 164;
This consent form will expire on (date)_____________ or __________ days from the. Only complete this form if you. This form will allow us to share certain health information about you with a family member or other trusted person. Sample authorization for release of confidential information.