Past Medical History Form
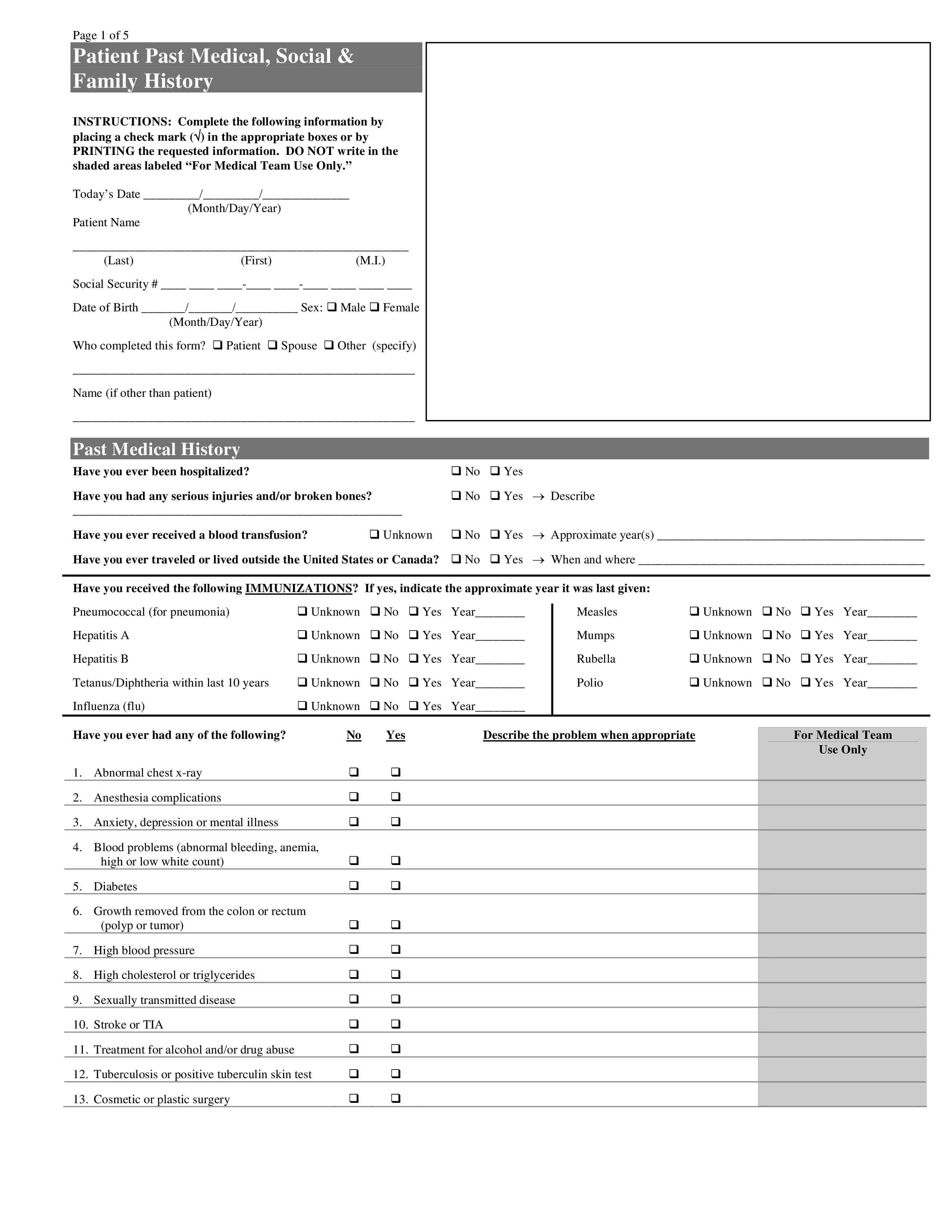
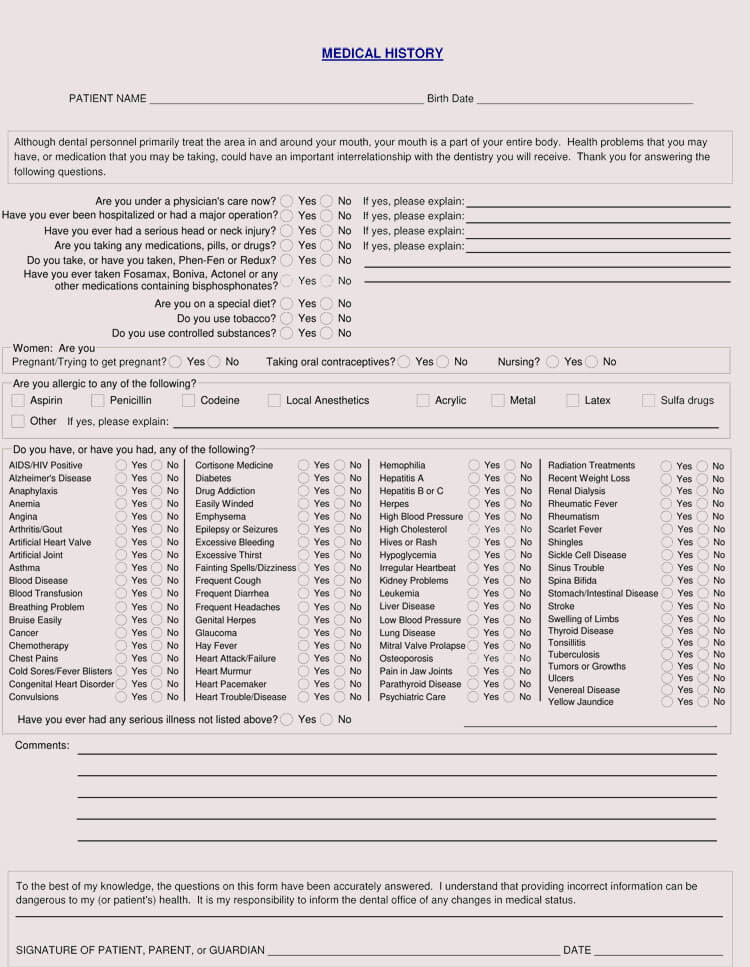
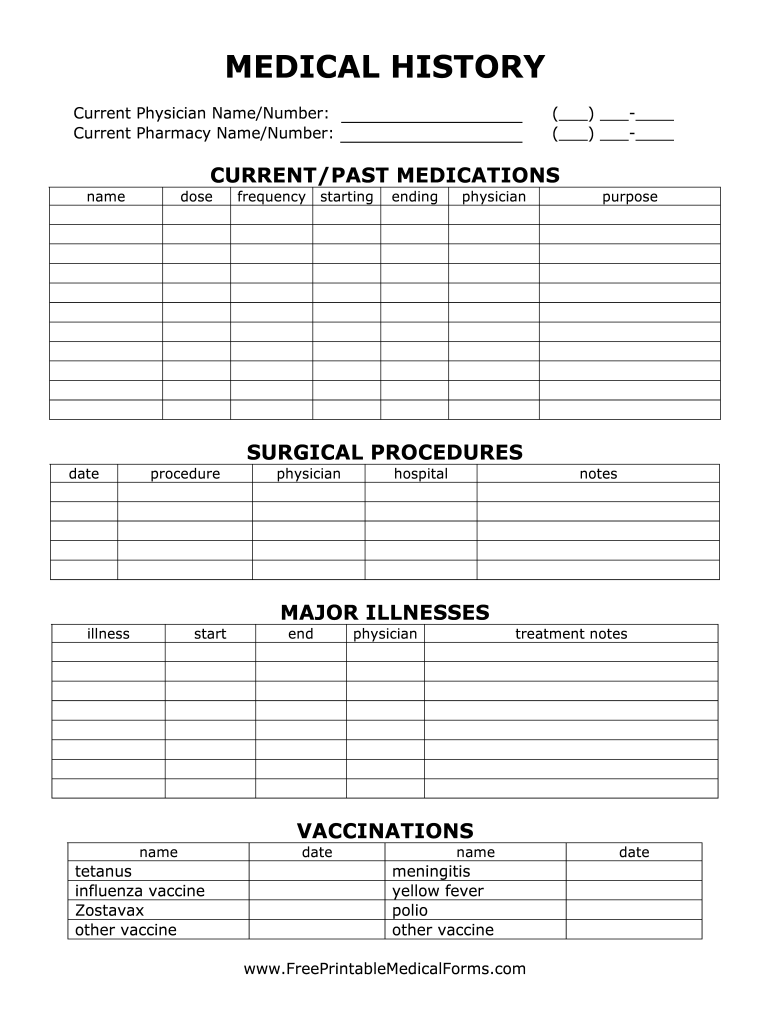
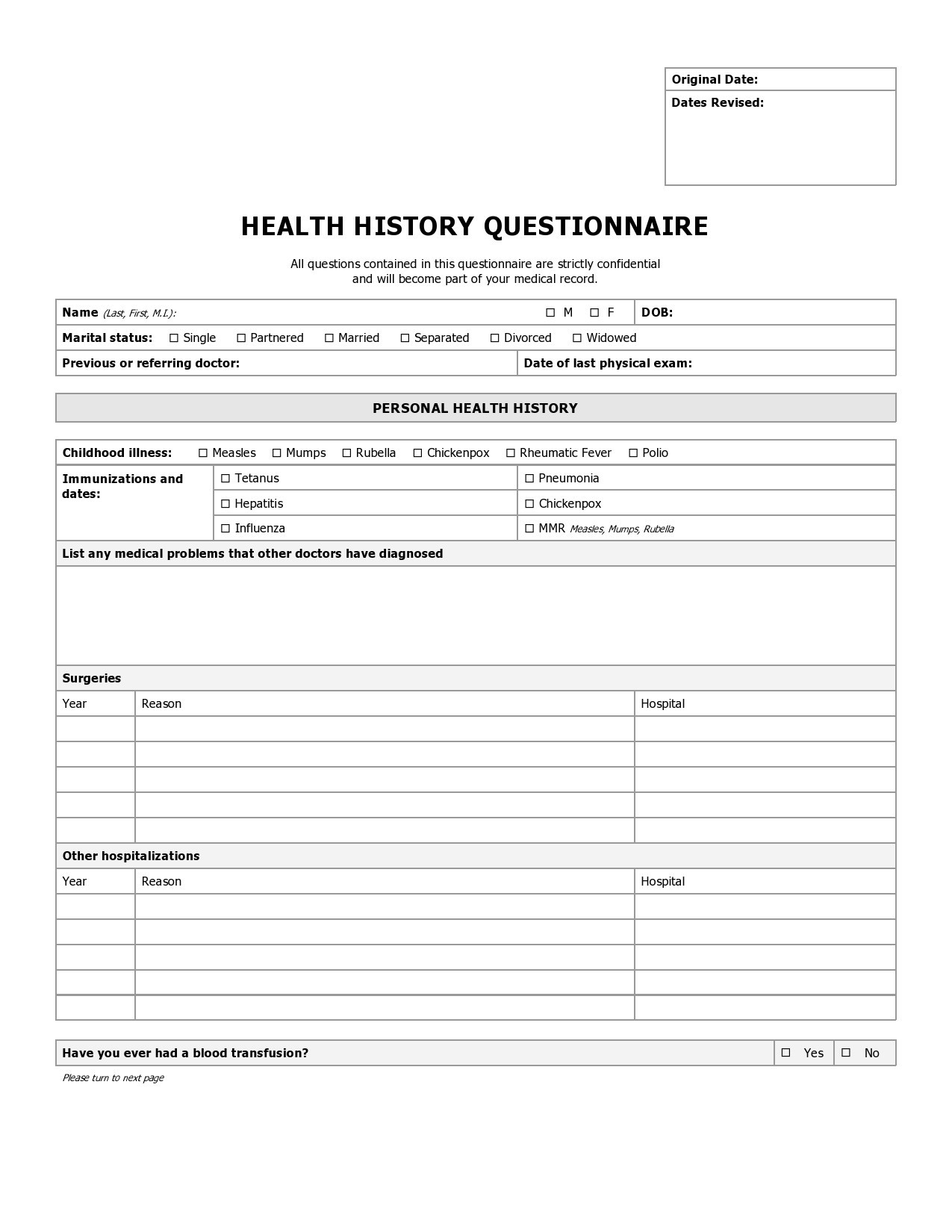
Past Medical History Form - List any specialists or other healthcare providers involved in your care. 08/13 page 1 of 2 full name: Patient name _____ past medical history date_____ please check any condition you have or have had. ☐no medical history to report. Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination.
Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. ☐no medical history to report. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. 08/13 page 1 of 2 full name: Patient name _____ past medical history date_____ please check any condition you have or have had. List any specialists or other healthcare providers involved in your care.
A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. Patient name _____ past medical history date_____ please check any condition you have or have had. Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. 08/13 page 1 of 2 full name: List any specialists or other healthcare providers involved in your care. ☐no medical history to report.
![67 Medical History Forms [Word, PDF] Printable Templates](https://printabletemplates.com/wp-content/uploads/templates/medical-history-form/medical history form 61-768x994.jpg)
67 Medical History Forms [Word, PDF] Printable Templates
List any specialists or other healthcare providers involved in your care. ☐no medical history to report. 08/13 page 1 of 2 full name: A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. Health history questionnaire your answers on this form will help your health care.
Past Medical History Form Templates at
☐no medical history to report. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. Patient name _____ past medical history date_____ please check any condition you have or have had. List any specialists or other healthcare providers involved in your care. 08/13 page 1 of.
Medical History Sheet Sample PDF Template
A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. 08/13 page 1 of 2 full name: ☐no medical history to report. List any specialists or other healthcare providers involved in your care. Patient name _____ past medical history date_____ please check any condition you have.

Past Medical History Form in Word and Pdf formats
☐no medical history to report. Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. List any specialists or other healthcare providers involved in your care..

Medical history form sample in Word and Pdf formats
Patient name _____ past medical history date_____ please check any condition you have or have had. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. ☐no medical history to report. Health history questionnaire your answers on this form will help your health care provider better.
![General Medical History Forms (100 Free) [Word, PDF]](https://www.wordtemplatesonline.net/wp-content/uploads/patient-Medical-History-Form-pdf.jpg)
General Medical History Forms (100 Free) [Word, PDF]
☐no medical history to report. Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. Patient name _____ past medical history date_____ please check any condition.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-09-scaled.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
List any specialists or other healthcare providers involved in your care. 08/13 page 1 of 2 full name: A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. Health history questionnaire your answers on this form will help your health care provider better understand your medical.
Printable Medical History Form Fill Online, Printable, Fillable
☐no medical history to report. 08/13 page 1 of 2 full name: List any specialists or other healthcare providers involved in your care. Patient name _____ past medical history date_____ please check any condition you have or have had. A general medical history form is a document used to record a patient’s medical history at the time of or after.
Free Medical History Form Template PRINTABLE TEMPLATES
Patient name _____ past medical history date_____ please check any condition you have or have had. List any specialists or other healthcare providers involved in your care. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. ☐no medical history to report. 08/13 page 1 of.
Patient Intake Medical History Form Fill Out, Sign Online and
Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. Patient name _____ past medical history date_____ please check any condition you have or have had. A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination..
List Any Specialists Or Other Healthcare Providers Involved In Your Care.
A general medical history form is a document used to record a patient’s medical history at the time of or after consultation and/or examination. 08/13 page 1 of 2 full name: Health history questionnaire your answers on this form will help your health care provider better understand your medical concerns and. Patient name _____ past medical history date_____ please check any condition you have or have had.