Cvs Caremark Prior Authorization Form
Cvs Caremark Prior Authorization Form - To access other state specific forms,. The requested drug will be covered with prior authorization when the following criteria are met: A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. • the requested drug will be used with a reduced calorie diet and increased physical activity to. I understand that any person who If a form for the specific medication cannot be found, please use the global prior authorization form. California members please use the california global pa form. Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. A physician will need to complete the form and. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the appropriate form and instructions on how to submit your request.
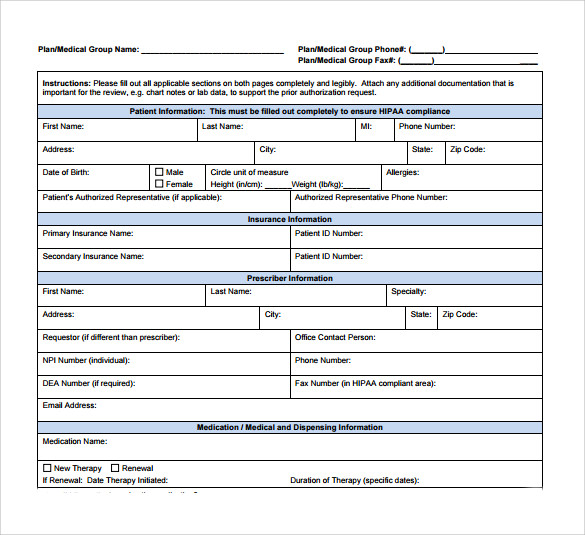
• the requested drug will be used with a reduced calorie diet and increased physical activity to. A physician will need to complete the form and. California members please use the california global pa form. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. If a form for the specific medication cannot be found, please use the global prior authorization form. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the appropriate form and instructions on how to submit your request. I understand that any person who To access other state specific forms,. The requested drug will be covered with prior authorization when the following criteria are met:
If a form for the specific medication cannot be found, please use the global prior authorization form. • the requested drug will be used with a reduced calorie diet and increased physical activity to. The requested drug will be covered with prior authorization when the following criteria are met: California members please use the california global pa form. To access other state specific forms,. Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. A physician will need to complete the form and. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the appropriate form and instructions on how to submit your request. I understand that any person who

Cvs Caremark Wegovy Prior Authorization Form
California members please use the california global pa form. Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. If a form for the specific medication cannot be found, please use the global prior authorization form. A physician will need to complete the form and. To access.

Free CVS/Caremark Prior (Rx) Authorization Form PDF eForms
Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. The requested drug will be covered with prior authorization when the following criteria are met: A physician will need to complete the form and. I understand that any person who If you wish to request a medicare.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
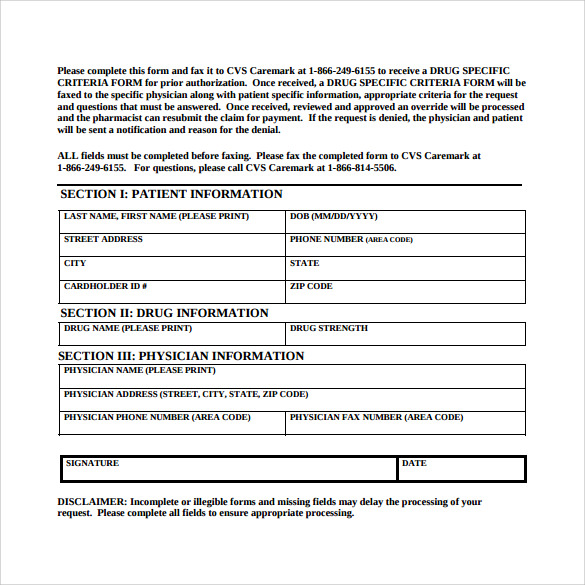
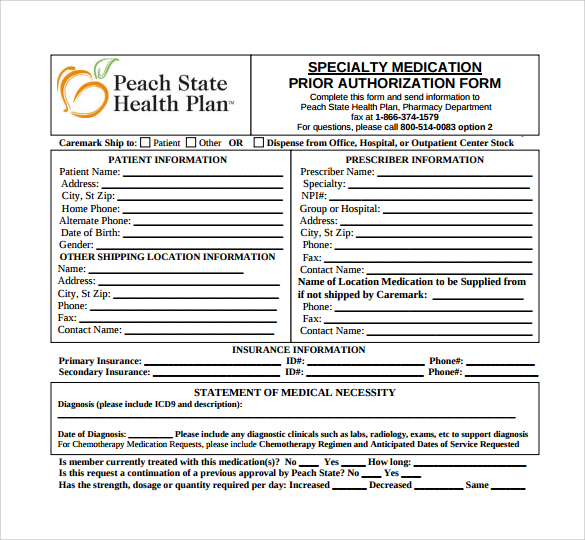
A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. The requested drug will be covered with prior authorization when the following criteria are met: California members please use the california global pa form. To access other state specific forms,. I understand that any person who
Sample Caremark Prior Authorization Form 8+ Free Documents in PDF
• the requested drug will be used with a reduced calorie diet and increased physical activity to. I understand that any person who Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. If a form for the specific medication cannot be found, please use the global.
Top Cvs Caremark Prior Authorization Form Templates free to download in
A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. To access other state specific forms,. A physician will need to complete the form and. California members please use the california global pa form. I understand that any person who

Caremark Electronic Pa Form 2017 Ncpdp airSlate SignNow
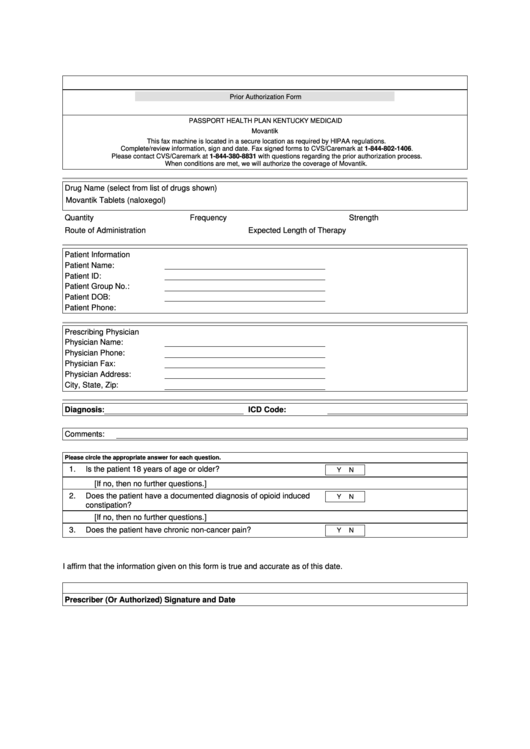
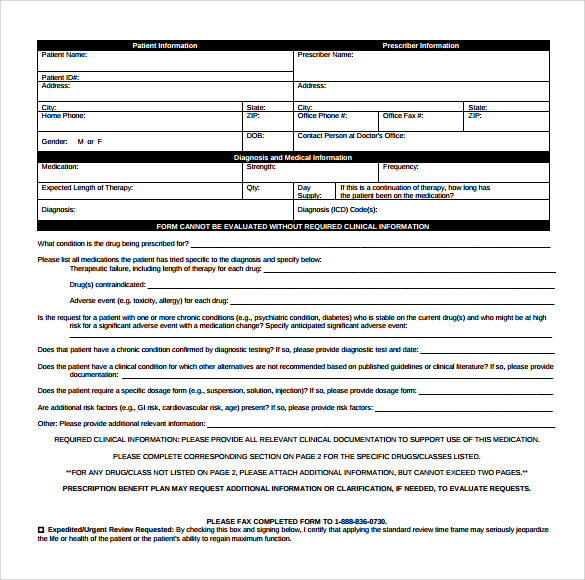
To access other state specific forms,. The requested drug will be covered with prior authorization when the following criteria are met: A physician will need to complete the form and. California members please use the california global pa form. If a form for the specific medication cannot be found, please use the global prior authorization form.
Sample Caremark Prior Authorization Form 8+ Free Documents in PDF
I understand that any person who If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the appropriate form and instructions on how to submit your request. California members please use the california global pa form. If a form for the specific medication cannot be found, please use the global.

Caremark Prior Authorization Request Form Fill and Sign Printable
• the requested drug will be used with a reduced calorie diet and increased physical activity to. A physician will need to complete the form and. I understand that any person who To access other state specific forms,. If you wish to request a medicare part determination (prior authorization or exception request), please see your plan’s website for the appropriate.

Cvs caremark prior authorization form Fill out & sign online DocHub
The requested drug will be covered with prior authorization when the following criteria are met: A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. To access other state specific forms,. California members please use the california global pa form. If you wish to request a medicare part determination (prior.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
California members please use the california global pa form. • the requested drug will be used with a reduced calorie diet and increased physical activity to. I understand that any person who If a form for the specific medication cannot be found, please use the global prior authorization form. If you wish to request a medicare part determination (prior authorization.
California Members Please Use The California Global Pa Form.
If a form for the specific medication cannot be found, please use the global prior authorization form. Information is available for review if requested by cvs caremark®, the health plan sponsor, or, if applicable, a state or federal regulatory agency. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. A physician will need to complete the form and.
If You Wish To Request A Medicare Part Determination (Prior Authorization Or Exception Request), Please See Your Plan’s Website For The Appropriate Form And Instructions On How To Submit Your Request.
To access other state specific forms,. • the requested drug will be used with a reduced calorie diet and increased physical activity to. I understand that any person who The requested drug will be covered with prior authorization when the following criteria are met: